- Diet
- Cancer
- Colorectal Cancer
- Prostate Cancer
- Breast Cancer
- Adenoid Cystic Carcinoma
- Amyloidosis
- Anal Cancer
- Appendix Cancer
- Astrocytoma - Childhood
- Ataxia-Telangiectasia
- Beckwith-Wiedemann Syndrome
- Bile Duct Cancer (Cholangiocarcinoma)
- Birt-Hogg-Dubé Syndrome
- Bladder Cancer
- Bone Cancer (Sarcoma of Bone)
- Brain Stem Glioma - Childhood
- Brain Tumor
- Breast Cancer - Inflammatory
- Breast Cancer - Metastatic
- Breast Cancer - Male
- Carney Complex
- Central Nervous System Tumors (Brain and Spinal Cord) - Childhood
- Cervical Cancer
- Childhood Cancer
- Cowden Syndrome
- Craniopharyngioma - Childhood
- Desmoid Tumor
- Desmoplastic Infantile Ganglioglioma, Childhood Tumor
- Ependymoma - Childhood
- Esophageal Cancer
- Ewing Sarcoma - Childhood and Adolescence
- Eye Melanoma
- Eyelid Cancer
- Familial Adenomatous Polyposis
- Familial GIST
- Familial Malignant Melanoma
- Familial Pancreatic Cancer
- Gallbladder Cancer
- Gastrointestinal Stromal Tumor - GIST
- Germ Cell Tumor - Childhood
- Gestational Trophoblastic Disease
- Head and Neck Cancer
- Hereditary Breast and Ovarian Cancer
- Hereditary Diffuse Gastric Cancer
- Hereditary Leiomyomatosis and Renal Cell Cancer
- Hereditary Mixed Polyposis Syndrome
- Hereditary Pancreatitis
- Hereditary Papillary Renal Carcinoma
- HIV/AIDS-Related Cancer
- Juvenile Polyposis Syndrome
- Kidney Cancer
- Laryngeal and Hypopharyngeal Cancer
- Leukemia - Acute Lymphoblastic - ALL - Childhood
- Leukemia - Acute Lymphocytic - ALL
- Leukemia - Acute Myeloid - AML
- Leukemia - Acute Myeloid - AML - Childhood
- Leukemia - B-cell Prolymphocytic Leukemia and Hairy Cell Leukemia
- Leukemia - Chronic Lymphocytic - CLL
- Leukemia - Chronic Myeloid - CML
- Leukemia - Chronic T-Cell Lymphocytic
- Leukemia - Eosinophilic
- Li-Fraumeni Syndrome
- Liver Cancer
- Lung Cancer - Non-Small Cell
- Lung Cancer - Small Cell
- Lymphoma - Hodgkin
- Lymphoma - Hodgkin - Childhood
- Lynch Syndrome
- Lymphoma - Non-Hodgkin - Childhood
- Lymphoma - Non-Hodgkin
- Mastocytosis
- Medulloblastoma - Childhood
- Melanoma
- Meningioma
- Mesothelioma
- Multiple Endocrine Neoplasia Type 1
- Multiple Endocrine Neoplasia Type 2
- Multiple Myeloma
- MUTYH (or MYH)-Associated Polyposis
- Myelodysplastic Syndromes - MDS
- Nasal Cavity and Paranasal Sinus Cancer
- Nasopharyngeal Cancer
- Neuroblastoma - Childhood
- Neuroendocrine Tumor of the Gastrointestinal Tract
- Neuroendocrine Tumor of the Lung
- Neuroendocrine Tumor of the Pancreas
- Neuroendocrine Tumors
- Neurofibromatosis Type 1
- Neurofibromatosis Type 2
- Nevoid Basal Cell Carcinoma Syndrome
- Oral and Oropharyngeal Cancer
- Osteosarcoma - Childhood and Adolescence
- Ovarian, Fallopian Tube, and Peritoneal Cancer
- Pancreatic Cancer
- Parathyroid Cancer
- Penile Cancer
- Peutz-Jeghers Syndrome
- Pheochromocytoma and Paraganglioma
- Pituitary Gland Tumor
- Pleuropulmonary Blastoma - Childhood
- Retinoblastoma - Childhood
- Rhabdomyosarcoma - Childhood
- Salivary Gland Cancer
- Sarcoma - Kaposi
- Sarcomas, Soft Tissue
- Skin Cancer (Non-Melanoma)
- Small Bowel Cancer
- Stomach Cancer
- Testicular Cancer
- Thymoma and Thymic Carcinoma
- Thyroid Cancer
- Tuberous Sclerosis Complex
- Unknown Primary
- Uterine Cancer
- Vaginal Cancer
- Von Hippel-Lindau Syndrome
- Vulvar Cancer
- Waldenstrom Macroglobulinemia (Lymphoplasmacytic Lymphoma)
- Werner Syndrome
- Wilms Tumor - Childhood
- Xeroderma Pigmentosum
- Veterans with Cancer
- Insurance and Cancer
- Prayers for Cancer Healing
- Prayers for Cancer Survival
- Pharmacology - Cancer Oncology drugs
- Natural Cures for Cancer
- Cancer Causing Foods
- Cancer Fighting Foods
- Kaposi Sarcoma
- Nausea and Vomiting in Cancer
- Adrenocortical Carcinoma
- Adolescents and Young Adults with Cancer
- Basal Cell Carcinoma of the Skin
- Burkitt Lymphoma
- Pancreatic Cancer
- Pain Management in Cancer
- CBD and Cancer Patients
- Cancer Treatment
- Stoma Bag
- Cancer Bra
- Cancer Wigs
- Lymphedema and Cancer
- Ductal Carcinoma In Situ (DCIS)
- Mouth Cancer
- Pregnancy and Breast Cancer
- Endometrial Cancer
- Heart Tumors, Childhood
- Merkel Cell Carcinoma
- Urethral Cancer
- Cancer in Young Adults
- Exercise and Cancer
- Insurance Denial and Cancer
- Bronchial Tumors
- Colostomy and Cancer
- Tube Feeding and Cancer
- Chronic Myeloproliferative Neoplasms
- Pulmonary Inflammatory Myofibroblastic Tumor
- Cutaneous T-Cell Lymphoma
- Fallopian Tube Cancer
- Breast Prostheses after Mastectomy
- Vascular Tumors
- Urethral cancer
- Music
Top videos




Lindsey Lyle, a physician assistant specializing in MPNs, reviews the lab tests that should be administered following an MPN diagnosis and how the results could affect overall care.
Lindsey Lyle is a physician assistant at the University of Colorado Cancer Center, specializing in hematological malignancies with a subspecialty in myeloproliferative neoplasms (MPNs). More about this expert here: https://www.uchealth.org/provi....der/lindsey-lyle--pa
Related Programs:
https://powerfulpatients.org/2....019/11/25/improving-
https://powerfulpatients.org/2....019/11/25/expert-tip
https://powerfulpatients.org/2....019/11/25/can-diet-a

Dr. Ruben Mesa welcomes Dr. Robyn Scherber, assistant professor in the Division of Hematology/Oncology and expert MPN specialist to the NCI-designated Mays Cancer Center at UT Health San Antonio MD Anderson Cancer Center. They discuss key MPN updates from the summer 2018 conferences of ASCO and The European Hematology Association (EHA), including new treatments, current clinical trials, and complementary approaches to the care of MPN patients. Follow Dr Mesa on twitter @mpdrc and the UT Health San Antonio Cancer Center @UTHealthCancer.
Learn more about our patient care, research and support at www.uthscsa.edu/patient-care/cancer-center


ABC News medical contributor Darien Sutton explains how a 53-year-old man was likely cured of HIV after a high-risk stem cell transplant.
WATCH the ABC News Live Stream Here: https://www.youtube.com/watch?v=w_Ma8oQLmSM
SUBSCRIBE to ABC NEWS: https://bit.ly/2vZb6yP
Watch More on http://abcnews.go.com/
LIKE ABC News on FACEBOOK https://www.facebook.com/abcnews
FOLLOW ABC News on TWITTER: https://twitter.com/abc
#ABCNLUpdate #DOJ #HIV #Groundbreaking #Treatment #Cured #HIVcure




This video is an excerpt from my one-day dermpath course in Paris, France, on October 8, 2021, for the Academie Internationale de Pathologie – Division Française (IAP French division).
Full 5 hour video of the entire course is available for free here: https://kikoxp.com/posts/8361.
WSI digital slide: https://kikoxp.com/posts/6679
Video discussing adenoid BCC vs adenoid cystic carcinoma here (at 41:31): https://kikoxp.com/posts/6682
Here's a case report we published about primary cutaneous adenoid cystic carcinoma (not the same case as this slide): https://pubmed.ncbi.nlm.nih.gov/25062259/
A complete organized library of all my videos, digital slides, pics, & sample pathology reports is available here: https://kikoxp.com/posts/5084 (dermpath) & https://kikoxp.com/posts/5083 (bone/soft tissue sarcoma pathology).
Please check out my Soft Tissue Pathology & Dermatopathology survival guide textbooks: http://bit.ly/2Te2haB
This video is geared towards medical students, pathology or dermatology residents, or practicing pathologists or dermatologists. Of course, this video is for educational purposes only and is not formal medical advice or consultation.
Presented by Jerad M. Gardner, MD. Please subscribe to my channel to be notified of new pathology teaching videos.
Follow me on:
Snapchat: JMGardnerMD
Twitter: @JMGardnerMD
Instagram: @JMGardnerMD
Kiko: https://kikoxp.com/profile/jer....ad_gardner1/content?
Facebook: https://www.facebook.com/JMGardnerMD/






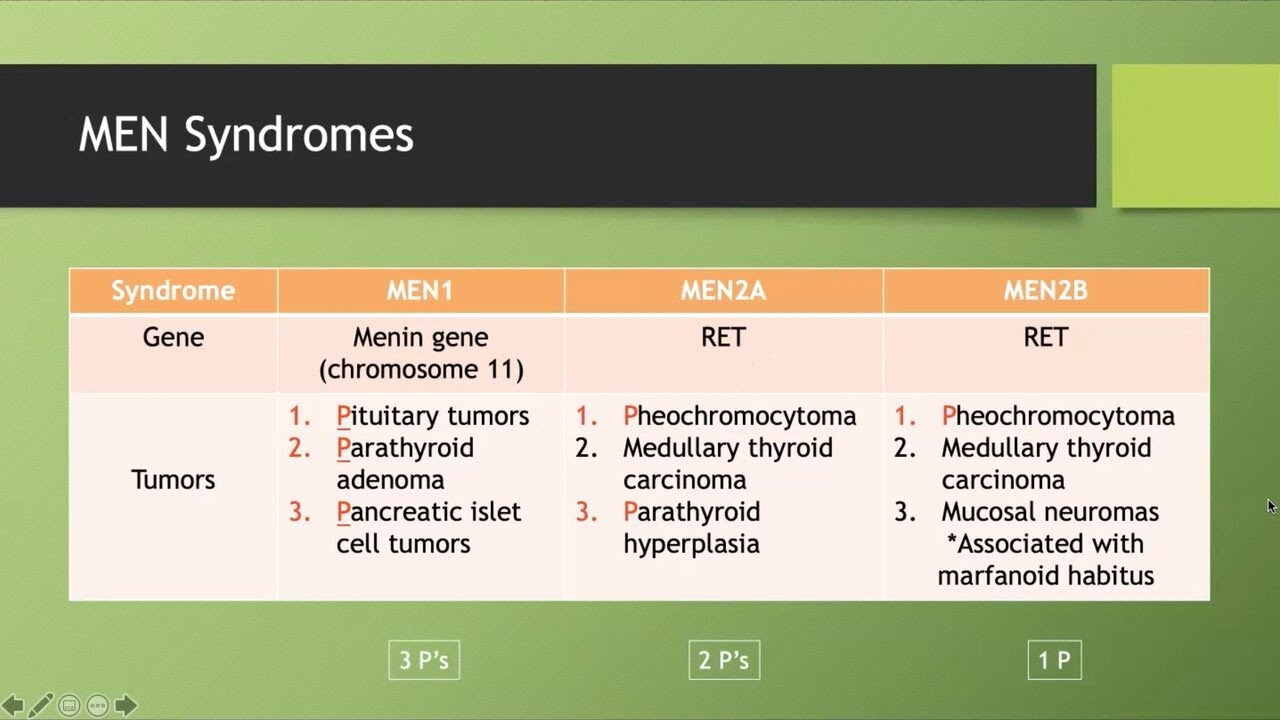
This video discusses the three most common MEN syndromes (MEN 1, MEN2A, MEN2B) by providing useful mnemonics as well as a brief explanation of commonly associated tumors (e.g., pheochromocytoma, medullary thyroid carcinoma).
This individual GI lecture video has been clipped directly from the comprehensive GI lecture series videos and may therefore contain errors associated with this process. You can find the “GI Lecture Series” playlist on the channel to watch the full lecture videos in their entirety.
Studying for board examinations can be daunting, with every resource offering a unique take on each medical condition. I created this channel to provide medical students - especially those studying for USMLE Step 1 and COMLEX Level 1 - with a "one-stop-shop" for medical content. For each lecture, I synthesized information from almost every major medical resource to provide you with a comprehensive and integrated lesson plan. I emphasize the pathophysiology of each disease so that you can leave each lecture with a detailed understanding of the material instead of memorizing hundreds of random facts.
All content discussed within the lecture series is designed for educational purposes only and should not substitute clinical judgment.
Original material in this lecture series may be redistributed provided that proper attribution is utilized. Please use “https://www.youtube.com/@doc.smoove” when attributing source material.
Errata:
Timestamps:
0:00 Overview
1:36 MEN1
2:33 MEN2A
5:57 MEN2B

Join Dr. Elizabeth Jaffee of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins for a Q&A discussion about immunotherapies in clinical trials for pancreatic cancer. #CRIsummit #Immunotherapy #pancsm https://www.cancerresearch.org/virtualsummit
There are limited effective treatments for most patients with advanced pancreatic cancer. It is the world's most lethal cancer and the fourth-leading cause of cancer-related death in the United States. Pancreatic cancer has taken the lives of Alex Trebek, Justice Ruth Bader Ginsberg, and civil rights activist Senator John Lewis. Pancreatic cancer patients are highly encouraged to seek clinical trials and many trials testing new immunotherapies are showing glimmers of hope. https://www.cancerresearch.org..../immunotherapy/cance
00:00 – Welcome from Tamron Hall
00:59 – Pancreatic Cancer and the Immune System
8:16 – Future of Cancer Immunotherapy
10:17 – Live Q&A
Dr. Jaffee begins the session with an overview of the characteristics of pancreatic cancer that allow it to hide from the immune system. There are three areas of research that are helping scientists understand how to awaken the immune system with immunotherapy: understanding how to bypass immune suppressive signals in the tumor microenvironment, understanding tumor heterogeneity, and developing quality T cells that have the ability to enter the tumor. Dr. Jaffee discussed promising clinical trials that combine immunotherapies with each other or other anti-cancer treatments to help induce a response to immune resistant tumors like pancreatic cancer.
Dr. Jaffe then address questions from the audience, including:
- What are some of the most common targets for vaccination?
- Is immunotherapy an immediate option? Is it generally recommended you undergo other types of anti-cancer treatments first?
- I would like to hear more about “compassionate use” and "off-label" use of immunotherapies in cancer. Is off-label access more commonly used in advanced stage cancers? What might be the criteria for use in non-advanced stage cancers?
- I lost my mother, brother, and aunt to pancreatic cancer. Why is pancreatic cancer so often diagnosed late? Are there any new early detection tests for pancreatic cancer?
- I would like to know if there is a role for immunotherapy in preventing recurrence, including after chemotherapy and/or after the Whipple procedure?
- Where can I find a pancreatic cancer immunotherapy clinical trial?
- What are common side effects of immunotherapy that your patients have experienced?
- Are there any tests to predict who might have a bad response to immunotherapy?
- Are you more susceptible to COVID-19 as a cancer patient?
- I am concerned about the safety of the new COVID-19 vaccines. Is it safe to get the vaccine if you have cancer?
- In your opinion, is telemedicine changing or potentially improving patient experiences on a clinical trial? How has your practice changed in the face of COVID-19?
Dr. Elizabeth M. Jaffee is an international leader in the development of immune-based therapies for pancreatic and breast cancers, specifically therapeutic vaccines. She is the Dana and Albert “Cubby” Broccoli Professor of Oncology at Johns Hopkins University, where she also serves as the deputy director of the Sidney Kimmel Comprehensive Cancer Center and the associate director of the Bloomberg~Kimmel Institute for Cancer Immunotherapy. She the past chair of the National Cancer Advisory Board for the National Cancer Institute, a past president of the American Association for Cancer Research, and was recently elected to the National Academy of Medicine. Dr. Jaffee has received numerous awards in recognition of her contributions, including CRI’s 2019 William B. Coley Award for Distinguished Research in Tumor Immunology. She is a member of the Cancer Research Institute Scientific Advisory Council and Clinical Leadership Team. https://www.cancerresearch.org..../about-cri/scientifi
Established in 1953, the Cancer Research Institute (CRI) is a 501(c)(3) nonprofit organization dedicated to harnessing our immune system’s power to control and potentially cure all cancers. Our mission: Save more lives by fueling the discovery and development of powerful immunotherapies for all types of cancer. To accomplish this, we rely on donor support and collaborative partnerships to fund and carry out the most innovative clinical and laboratory research around the world, support the next generation of the field’s leaders, and serve as the trusted source of information on immunotherapy for cancer patients and their caregivers. https://www.cancerresearch.org
Cancer Research Institute is a registered 501(c)(3) nonprofit under EIN 13-1837442. Donations are tax-deductible to the fullest extent allowable under the law.
sync ID: MB01WB7EUVJUBPT


