Surgeon explains melanoma surgery

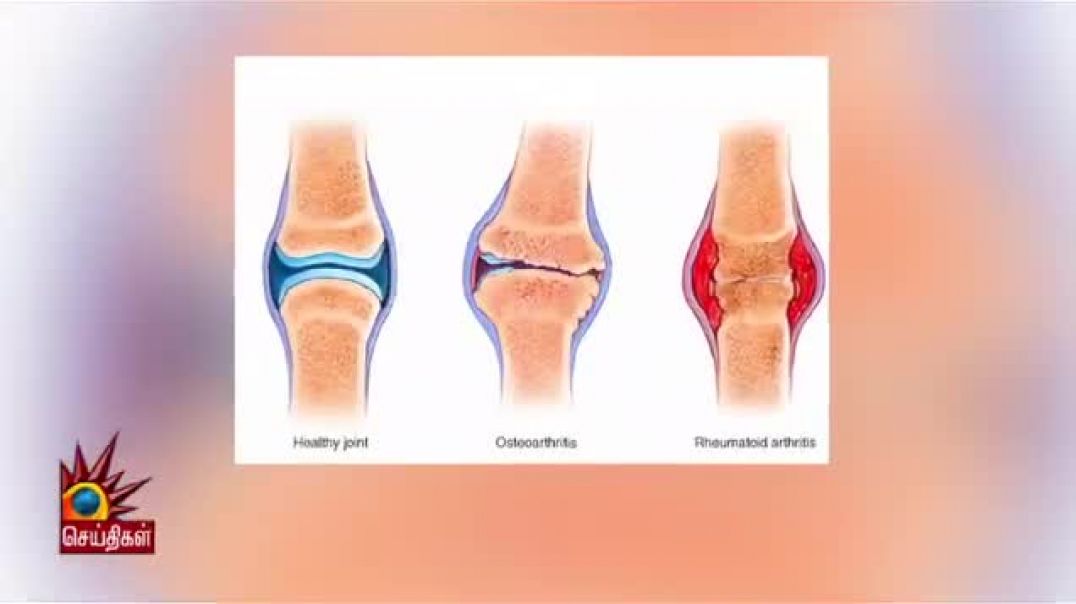
Surgical oncologist explains what melanoma is, what we need to know about it, and how we excise it from the skin. Melanoma skin cancer is the 5th most common cancer in the US. Melanoma is a skin cancer that comes from the melanin producing cells called melanocytes. These cells are in the lower layer of the skin and produce the pigment melanin that turns your skin dark. A normal mole is a cluster of non-cancerous melanocytes. Melanoma means that these melanin-producing cells have become cancerous. Melanoma is only 5% of all skin cancers. The other types of skin cancer such as squamous cell skin cancer and basal cell skin cancer are much more common but are not as dangerous. Risk factors for melanoma are having red hair/blond hair, green or blue eyes, and a history of multiple sun burns. It can happen at any age even in teenagers and young adults. Most melanoma grow from pre-existing moles. If a mole is changing with (A) for asymmetric margins (B) borders that are ragged (c) colors are different or changing or (d) diameter is more than a pencil-eraser and growing then this could be a sign of melanoma. A doctor will biopsy any concerning skin lesions with these characteristics. Once the suspicious mole is biopsied it is sent to a pathology doctor. The pathology doctor needs to tell us if the mole is a cancerous melanoma, and if it is a melanoma we want to know how deep it is growing down into the skin. We also want to know if the most superficial layer of skin over the melanoma is gone which is a factor called ulceration. Ulceration of a melanoma is a sign that is more aggressive so it’s a bad thing.
The most common form of melanoma is melanoma in-situ. In-situ means that the melanoma cells are stuck in the most superficial part of the skin and have not spread down into the skin layer. These tend to spread out in the skin and the edges can be very hard to see. (picture) Even though the melanoma cells have not grown deep, we still remove the full thickness of the skin down to the fat under the skin. Melanoma cells also spread out into the skin and we always want a margin of normal skin around a melanoma to be sure we also remove these few satellite cells. For melanoma in-situ we need to remove 5 mm from the visible edge of the melanoma. If the melanoma is about 1 cm in size, then taking 5 mm in every direction around it leaves a 2 cm hole. In order to close a hole in the skin that is 2 cm in diameter we can’t just stitch it together because the edges will lump up and it just won’t look good. Surgeons usually make an ellipse shape that is about 3x as long as it is wide and when we stitch this shut it will be a nice flat line. So for the 2 cm in diameter hole we make a 6 cm long elliptical excision.
The next form of melanoma is considered invasive down into the skin. If the depth of invasive melanoma is less than 1 mm from the surface of the skin this is called a thin melanoma. For a thin melanoma, we want to go 1 cm out from the edge of the visible melanoma in every direction. For a 1 cm in diameter melanoma, this means that the excision hole is 3 cm in diameter. The ellipse of skin removed to close this in a flat line is then 3 x as long so 9 cm in length. Any melanoma deeper than 1 mm and up to 4 mm in depth is called an intermediate thickness melanoma. Any melanoma deeper than 4 mm in depth is called a thick melanoma. The deeper a melanoma gets the more dangerous it is as far as the ability to spread or metastasize and regrow. But from a surgeon perspective, we usually treat intermediate and thick melanoma the same. We recommend removing 2 cm in every direction from the edge of the melanoma. These holes can get pretty big. For a 1 cm in diameter melanoma, a 2 cm margin in every direction will result in at least a 5 cm hole in diameter. We also recommend removing the entire thickness of the skin and the underlying fat tissue all the way down to the muscle underneath for these melanomas. To close the skin in a straight line for a 5 cm in diameter hole, the ellipse will be 15 cm long, this is 6 inches. This requires that we lift the skin up off it’s attachments to the underlying muscle for 5-10 cm off to the sides of the cut. This releases the tension so that the edges of the skin can be pulled together with stitches again. This leaves a large pocket under the closure.
Melanoma can spread to lymph nodes. Lymph nodes are part of your immune system and are attached to channels that lay just under the skin called lymphatic channels that carries lymphatic fluid. Melanoma deeper than 1 mm can have cells break off into the lymphatic fluid and get carried to the lymph nodes where they get stuck and grow. The technique to check the lymph nodes is called a sentinel lymph node biopsy and I have a separate talk on that you should check out. Anytime we have a melanoma deeper than 1 mm or a thin melanoma that is ulcerated we consider checking the sentinel lymph node biopsy.
-
Category



















No comments found